

Applying the Plan-Do-Study-Act Cycle to Improving Patient Experience
F
How can you use the Plan-Do-Study-Act (PDSA) cycle (Figure 1) to improve patient experience?
- Plan – Decide on your goals, strategies, and actions.
- Do – Move forward in implementing your plans.
- Study – Test and monitor your progress.
- Act – Expand the improvements to more areas within your healthcare system.
Figure 1. Plan-Do-Study-Act (PDSA) Cycle
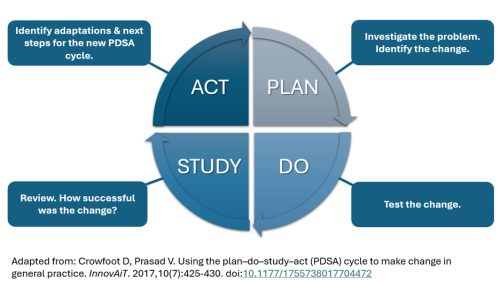
Adapted from: Crowfoot D, Prasad V. Using the plan–do–study–act (PDSA) cycle to make change in general practice. InnovAiT. 2017,10(7):425-430. doi:10.1177/1755738017704472
This topic brief reviews what you and/or your team can do at each step of the cycle.1 Keep in mind that you may repeat this PDSA cycle several times, implementing one or more interventions on a small scale first and then expanding to broader actions based on lessons from the earlier cycles.
Plan: Develop Goals and an Action Plan
There are four key steps in the planning stage of a PDSA cycle:
- Establish improvement goals.
- Identify possible strategies.
- Choose specific interventions to implement.
- Prepare a written action plan.
1. Establish Goals for Improving Patient Experience
The team's first task is to establish one or more aims or goals for the improvement work. By setting clear, measurable goals, you will be better able to communicate your objectives to all of the sectors in your organization that you might need to support or help implement the intervention.
Each goal should reflect a specific aspect of patient experience that the team is targeting and be both measurable and feasible.2 As a tool for measuring patient experience, the AHRQ Consumer Assessment of Healthcare Providers and Systems (CAHPS) surveys offer a validated way to assess the impact of changes. However, since there is typically a lag between the implementation of changes, the impact on people's experiences, and the assessment of that impact with a CAHPS survey, your team needs to define both ultimate goals as well as incremental objectives that can be used to gauge short-term progress.
![]() Related topic brief: Read about comparing scores with benchmarks in How To Analyze CAHPS Survey Results: An Overview of Three Options.
Related topic brief: Read about comparing scores with benchmarks in How To Analyze CAHPS Survey Results: An Overview of Three Options.
- Start by defining your ultimate goals. For example, goals for the CAHPS Clinician & Group Survey could include—
- An X percentage-point increase in the score for the "Getting Timely Appointments, Care, and Information" composite measure (scaled 0–100)
- An X percentage-point increase in the overall rating of the provider (scaled 0–100)
- Equaling or surpassing the mean score for the “Provider Communication” composite measure for other primary care clinics in your health system, state, or region
- Then ask, "What is the gap between our current state and our goals?"
- This is the assessment of your current scores (i.e., where your performance is currently) to your goal scores (i.e., what you would like your performance to be)
- Make a list of those gaps or desired improvements in performance on specific metrics and use them to make SMART (specific, measurable, achievable, realistic, and timebound) incremental objectives. For example—
- Reduce the number of days it takes to get an appointment for nonurgent and urgent visits by Y percent each quarter, which would reduce the measured access issues for nonurgent and urgent visits.
- Reduce the monthly number of complaints for individual medical groups or a health plan.
 Learn more:
Learn more: 2. Identify Possible Strategies
With objectives in place, the next task is to identify possible strategies or interventions and select one that seems promising. There are many sources for new ideas or different ways of doing things both within and outside of the healthcare industry.
New ideas and innovative solutions can be found—
- At conferences or workshops.
- In academic literature and other publications (Review examples of academic literature focused on patient experience improvement interventions).
- Through patients and their families—whether through patient narratives, direct interviews, and focus groups, as partners on quality improvement teams, or as members of Patient and Family Advisory Councils.
"Ideas for change can come from a variety of sources: critical thinking about the current system, creative thinking, observing the process, a hunch, an idea from the scientific literature, or an insight gained from a completely different situation. A change concept is a general idea with proven merit and sound scientific or logical foundation that can stimulate specific ideas for changes that lead to improvement."
Plsek P. Innovative thinking for the improvement of medical systems . Ann Intern Med 1999;131:438-44.
3. Choose Specific Interventions To Implement
To decide which new ideas or benchmark practices to implement, consider several factors:
- Fit with the problem. The best intervention will be one that suits the specific problem you need to address (or can be tailored as needed). To ensure a good fit, seek input from both affected staff as well as patients or health plan members. If you ignore either source of information in your planning, you may choose an intervention that will not fix the actual problem.
- Technical merit. The ideas most likely to be adopted provide significant advantages over existing practices for both patients and providers—whether in the form of increased efficiency, higher patient and employee satisfaction, or improved outcomes. All improvement efforts ultimately must answer the question, "What's in it for me?"
- Compatibility with the organization and local culture. Serving Cuban coffee in the waiting rooms of Miami-based clinics may be very patient friendly, but is not likely to be viewed with the same enthusiasm by patients in Arizona or Massachusetts.
Depending on the nature of the intervention, you may want to break it down into a set of related but discrete changes. Your intervention may include a training element, efforts to inform and motivate key stakeholders, development of workflows or protocols to implement, and dissemination of information regarding the new and old processes. For example, if the team decides to implement a new specialist referral process, you could begin by making changes to the procedures used to communicate with the specialist's office (either within the system’s electronic health record (EHR) or with an outside specialist referral). The communication process with the health plan might then be the target of a separate change.
4. Prepare a Written Action Plan
Although there is no one "correct" way to write an action plan for your organization or facility, it is important to have some form of written document that states your goals, lists your overall strategies to achieve those goals, and then delineates the specific actions you will take to implement the interventions you have selected.
![]() How do you begin?
How do you begin?
Visit the Resource Library for an action plan template (Word, 43 KB; PDF, 264 KB) you can adapt to your improvement project.
Related resource: A PDSA worksheet from the Virginia Mason Institute.
One way to organize the action plan is to review the following key questions and briefly document your answers:
- What area(s) do you want to focus on for improvement?
- What are the goals?
- What initiative(s) and specific actions will you implement?
- Who will be affected and how?
- Who will lead/champion the initiative and manage the project?
- What resources will be needed?
- What are possible facilitators to change? How can we incorporate those?
- What are possible barriers and how can they be overcome? Read more about barriers below.
- How will you measure progress and success? It is important to specify the measures you will use to monitor progress in achieving the desired changes to organizational processes and CAHPS scores.
- What is the timeline? Record your planned start and end dates for each action. It can help to use a Gantt chart format to verify that the timing of sets of actions makes sense and is feasible to complete with the staff you have available.
- How will you share your action plan?
- To the extent that the improvement initiative was successful, what will it take to sustain the improvements over time?
- Does the improvement initiative need to be spread across other areas of healthcare (such as other clinics, other hospital departments or hospital units, or other facilities)?
![]() Related topic brief: Read about Using Measures To Monitor Progress.
Related topic brief: Read about Using Measures To Monitor Progress.
Identify and Address Barriers to Change
Barriers to improvement come in many guises. As part of the planning process, an improvement team will need to take a hard look at the psychological, physical, and procedural barriers it has to address in order to accomplish its aim.
Psychological barriers such as fear of change, fear of failure, grief over loss of familiar processes, or fear of loss of control or power can be significant impediments to overcome. An improvement process often requires significant changes in people's attitudes and behaviors; you may be asking staff to give up their old standards and practices and adopt new ones. While many staff will "get it" early and pitch in enthusiastically, you can expect pushback from some staff as you introduce new processes and habits.
Other common barriers include the following:
- Lack of basic management expertise.
- Lack of training in customer service, quality improvement methods, or clinical areas such as doctor-patient communication.
- Inadequate staffing levels.
- Poor information technology systems.
- Outdated or misguided organizational policies. For example, many organizations are so concerned about violating HIPAA regulations that they do not want to give information to a patient about their own care for fear of violating patient confidentiality.
Despite the serious nature of some of these barriers, few are large enough to bring a project to a halt. Typically, they are cited as excuses for two of the fundamental barriers to change: fear of new ways of doing things and fear of failure. It is important to remember that introducing and reinforcing changes in behavior that "stick" in the form of sustainable practices will take some work and time to succeed. Over time, as less enthusiastic staff see positive progress, they too will become more engaged and supportive.
Cultivate Facilitators of Change
As part of the action plan, the team also needs to identify factors that could facilitate their work. Facilitators can include financial or nonfinancial incentives, such as gain sharing for staff if a specific target is met or better quality of life for the staff when a problem is fixed. Other facilitators include picking an aim that is part of the organization's strategic plan or one that will improve other goals the staff care about, such as clinical outcomes.
Sometimes, an important facilitator of change is the ability of that change to help achieve secondary goals. For example, improvements in doctor-patient communication may decrease medication errors, or the development of shared care plans may reduce no-shows for appointments or procedures.
Do: Implement and Refine Actions on a Small Scale
Once you have selected interventions, the next stage of the cycle is to develop, test, and refine specific changes. It helps to think of this stage as a number of "mini-cycles" within the larger improvement cycle, in the sense that the microsystem or team is likely to go through multiple iterations of testing and refining before the specific changes add up to a real intervention. A microsystem is a self-contained subsystem located within a larger system; it generally constitutes the smallest unit of analysis in systems theory.
Mini-Cycles of Improvement
Small-scale tests of the interventions you wish to implement help refine improvements by incorporating targeted modifications over time. The targeted modifications may be implementing a change within a given unit or set of units, or one work process within a clinic that is broadened to more clinics (same work process), or a change with a selected group of staff. Which change depends on the chosen area of improvement, but the principle of starting small, testing the change, and repeating after modifying the change remains the same. Conducting these tests of change within a microsystem can be very powerful in the following ways:
- They allow for incremental modifications of interventions to fix problems, which helps the larger implementation run smoothly.
- Failures are low risk because you have not tried to change the entire culture.
- You create enthusiasm and positive "word of mouth" for early successes.
- It is easier to accumulate evidence for implementation when people are engaged in making something work rather than focused on the "failure analysis."
Most improvement strategies require some adaptation to the culture of the organization. Frontline staff will frequently resist new ideas if they are not allowed to modify the strategies and test their own ideas. Room for this modification can be built into the small-scale repeated tests over time. Also, patient-centered improvement strategies have to consider the needs of patients and their families as well as the staff. Building in ways to collect feedback from patients and families and building their ideas and feedback for improvement into the process of the repeated tests over time is recommended. This accommodation allows for codesign of the change among staff, patients, and families.
Visit the Resource Library to review key articles on implementing and sustaining innovations in healthcare settings.
Study: Monitor Progress
This stage, which is interwoven with the “Do” stage,” involves evaluating the intervention to improve patient experience against the improvement goals using the measures established for tracking progress. Here are some questions to ask:
- Is the intervention reducing the time required to see a specialist?
- Are health plan members reporting better experiences with regards to getting care quickly?
In this phase, it is important to gain feedback from staff, patients, and families concerning what is working or not working so that the strategies can be modified and changed for the next cycle of testing.
Act: Expand Implementation To Achieve Systemwide and Sustainable Improvement
Building off of the development, testing, and refinement of specific changes, the final stage of the PDSA cycle involves adopting a successful intervention to improve patient experience more broadly across and within the organization. There are no set rules about how long this part of the cycle takes, nor about how many implementation phases or steps are needed for systemwide implementation.
It is equally important to focus on sustaining the improvements made during the PDSA cycles. Ongoing measurement, whether monthly or quarterly, is critical to—
- Ensuring that the organization continues to make progress toward achieving and sustaining improvement aims.
- Identifying barriers to dissemination and issues in need of further analysis.
One key element of the “Act” step that is often neglected is the communication of successes throughout the organization—to organizational leaders as well as clinical and administrative staff. By discussing successful projects, the team helps reinforce the culture of quality improvement, build credibility for the intervention, reward those involved, and foster the spread of effective innovations.
How leaders can communicate about successes within an organization
- Use media and interpersonal communication to promote the work of specific improvement teams.
- Highlight successful innovations in regular staff touchpoints, such as newsletters and other regular communications and in staff and board meetings.
- Reinforce the importance of the project by sitting in on improvement team meetings or visiting the practice site or unit involved in the project.
A related practice is the communication of change beyond the walls of the organization to members or patients. By telling people about innovative practices, you can raise the standard of expectations—whether through regular external meetings, conferences, newsletters, emails, office computer screensavers in exam rooms or hospital waiting rooms, member websites, or handouts in the office. Be creative about ways to get the word out about the improvements. Remember also to share the information with the staff and the patients and family members who provided feedback in the process; they also may have ideas about sharing the results.
1. This topic brief uses “you” to refer to the reader as an individual and/or the reader’s team.
2. Katakam L, Suresh GK. Identifying a quality improvement project. J Perinatol 2017 Oct;37(10):1161-65. doi: 10.1038/jp.2017.95. Epub 2017 Aug 24. PMID: 28837135.